
D322. ADULT SAFEGUARDING
{{org_field_logo}}
{{org_field_name}}
D322. ADULT SAFEGUARDING
Scope
Part 1 Policy Statement Index
1.0 Policy Statement
1.1 Multi-Agency Safeguarding (Adults) Protocol
2.0 Care Act
2.1 Definition of Vulnerable Adult
2.2 Adult Safeguarding, what it is and why it matters
2.3 Safeguarding is not a substitute for:
2.4 The Care Act requires that all each Authority must
2.5 Aims of Adult Safeguarding
2.6 The Six Principles that underpin all Adult Safeguarding
2.7 Case Study
3.0 Types of Abuse and Neglect
3.1 Patterns of Abuse
3.2 Who Abuses and Neglects Adults
3.3 Spotting signs of Abuse and Neglect
3.4 Case Study
4.0 The Mental Capacity Act 2005
5.0 Reporting and responding to Abuse and Neglect
6.0 Local Authority’s role in carrying out enquiries
6.1 Information Gathering Diagram
6.2 Decision making Tree
7.0 Procedures for responding in individual cases
7.1 When should an enquiry take place
7.2 Who can carry out an enquiry
7.3 Case Study
7.4 What happens after an enquiry
7.5 Safeguarding Plans
8.0 Information Sharing
8.1 Record Keeping
8.2 Confidentiality
8.3 Front Line Staff
9.0 Safeguarding Adults Boards (SABs)
9.1 Safeguarding Adults Reviews (SAR)
Part 2 The Policy Index
10.0 Making Enquiries –
10.1 Staff – How to Report a Safeguarding Concern – name of Designated Safeguarding Lead
10.2 Service Users – How to Report a Safeguarding Concern
10.3 The Role of the Manager
10.4 The Role of the Local Authority
11.0 Statutory Notifications to CQC
12.0 Restrictive Interventions
- Related Policies
- Related Guidance
- Contact List
- Training Statement
1.0 Policy Statement
Safeguarding is everyone’s business and responsibility irrespective of what roles they may undertake within the company.
Protecting an adult’s right to live in safety, free from abuse and neglect. It is about people and organisations working together to prevent and stop both the risks and experience of abuse or neglect, while at the same time making sure that the adult’s wellbeing is promoted including, where appropriate, having regard to their views, wishes, feelings and beliefs in deciding on any action. This must recognise that adults sometimes have complex interpersonal relationships and may be ambivalent, unclear or unrealistic about their personal circumstances.
- People with care and support needs, such as older people or people with disabilities, are more likely to be abused or neglected. They may be seen as an easy target and may be less likely to identify abuse themselves or to report it.
- People with communication difficulties can be particularly at risk because they may not be able to alert others.
Sometimes people may not even be aware that they are being abused, and this is especially likely if they have a cognitive impairment. (SCIE June 2021)
With the introduction of the Care Act 2014 changes came into place, which updated adult safeguarding in England. This adult safeguarding guidance replaced “No Secrets” in its entirety. New safeguarding duties apply to an adult who:
• Has need for care and support (whether or not the local authority is meeting any of those needs; and
• Is experiencing, or at risk of abuse or neglect; and
• as a result of those care and support needs is unable to protect themselves from either the risk of, or the experience of abuse or neglect
The above duties have a legal effect in relation to organisation other than the local authority e.g. the NHS or Police.
The company Safeguarding Lead is {{org_field_registered_manager_first_name}} {{org_field_registered_manager_last_name}}, (Registered Manager).
1.1 Multi-Agency Safeguarding (Adults) Protocol
All local authorities will update their multi-agency safeguarding agreement to reflect these changes. Given the location of the office this sits within the your local authority Adults Safeguarding Area Please refer to this link to find the contact details of our local Adult Safeguarding Authority: {{org_field_local_authority_information_link}}
Phone number for our local Adult Safeguarding Authorty: {{org_field_local_authority_phone_number}}
All Local Authorities are required to produce the above Guidance. When contracted with more than one authority we ensure all protocols are listed and followed.
2.0 Care Act 2014
The changes introduced in April 2015 are fully detailed in the Care and Support Statutory Guidance issued under the Care Act 2014 (Chapter 14) of the Act. This replaces current guidance and covers the following:
• Adult safeguarding, what it is and why it matters
• Abuse and neglect
- what they are and spotting the signs
- reporting and responding to abuse and neglect
• Carers and adult safeguarding;
• Adult safeguarding procedures;
• Local authority’s role and multi-agency working;
• Criminal offences and adult safeguarding;
• Safeguarding enquiries;
• Safeguarding Adult Boards; (SABs)
• Safeguarding Adults Reviews (SARS);
• Information sharing, confidentially and record keeping;
• Roles responsibilities and training in local authorities, the NHS and other agencies.
The government have also re – issued the Care and Support Statutory Guidance May 9th 2016 issued under the Care Act
We are aware of the changes within chapter 14 in particular relation to Local Authorities roles and responsibilities
Please note:
Where someone is 18 years old or over but whose services are arranged via children services any safeguarding issue is dealt with via the adult safeguarding arrangement within the local authority or other statutory partner such as NHS or Police.
2.1 Definition of Vulnerable Adult
The term “vulnerable adult” is in itself contentious. By labelling adults “vulnerable” there is a danger that they will be treated differently.
The label can be stigmatising and result in assumptions that an individual is less able than others to make decisions and to determinate the cause of their lives. In this way, the term can level to subtle forms of in appropriate discrimination. Throughout this policy the distinction between adult with the capacity to make decisions and adults lacking capacity is emphasised. Adults who have capacity retain the right to make their own decisions and to direct their own lives. Adults lacking capacity to make decisions, though they retain the right to be involved in decision – making as far as possible nevertheless require decisions to be made on their own behalf and the overall approach shifts to promoting their best interests. The judgement that an adult is vulnerable should not be confused with a decision about their capacity. They are distinct questions although a lack of capacity will, ordinarily, contribute to an adult’s vulnerability.
2.2 Adult safeguarding, what it is and why it matters:
- It is a means of protecting an adult’s safety, free from abuse and neglect. It means people and organisations working together to prevent and stop such abuse and neglect, whilst making sure that the adult’s wellbeing is promoted, including, where appropriate, due regard to their views, wishes, feelings and beliefs in deciding on any action. This must recognise that adults sometimes have complex interpersonal relationships and may be ambivalent, unclear or unrealistic about their personal circumstances.
- Organisations should always promote the adult’s wellbeing in their safeguarding arrangements. People have complex lives and being safe is only one of the things they want for themselves. Professionals should work with the adult to establish what being safe means to then and how that can best be achieved. Professionals should not be advocating “safety” measures which do not take account of individual wellbeing as defined in chapter 1 of the Care and Support Statutory Guidance issued by the Department of Health.
2.3 Safeguarding is not a Substitute for:
- Providers responsibilities to provide safe and high-quality care and support;
- Commissioners regularly assuring themselves of the safety and effectiveness of commissioned services;
- The Care Quality Commission (CQC) ensuring that regulated providers comply with the fundamental standards of care or by taking enforcement action; and
- The core duties of the Police to prevent and detect crime and protect life and property
2.4 The Care Act requires that each authority must:
- Make enquiries or cause others to do so, if it believes an adult is experiencing, or is at risk of abuse or neglect. An enquiry should establish whether any action needs to be taken to prevent or stop abuse or neglect, and if so by whom;
- Set up a Safeguarding Adults Board (SAB);
- Arrange where appropriate, for an independent advocate to represent and support an adult who is the subject of a safeguarding enquiry or Safeguarding Adult Review (SAR) where the adult has substantial difficulty in being involved in the process and where there is no other suitable person to present and support them;
- Co-operate with each of its relevant partners in order to protect the adult. In their turn each relevant partner must co-operate with the local authority.
2.5 Aims of Adult Safeguarding
The Act sets out the following which apply to all local authorities and their relevant partners. Relevant partners include NHS, Police, Ambulance Service. Regulated or unregulated providers and all parties involved in the enquiry;
- Stop abuse or neglect wherever possible
- Prevent harm and reduce the risk of abuse or neglect to adults with care and support needs
- Safeguard adults in a way that supports them in making choices and having control about how they want to live;
- Promote an approach that concentrates on improving life for the adults concerned;
- Raise public awareness so that communities as a whole, alongside professionals, play their part in preventing, identifying and responding to abuse and neglect;
- Provide information and support in accessible ways to help people understand the different types of abuse, how to stay safe and what to do to raise a concern about the safety or well-being of an adult; and
- Address what has caused the abuse or neglect.
The Care Act sets out the steps which local authorities must implement in order to meet the legal requirements of the Act. It is imperative that all staff become familiar with these requirements. Guidance developed by our local authority partners will be included in this policy as it becomes available. All Local Authorities will review and amend the Multi-Agency Safeguarding Protocol which is available from the Local Authorities safeguarding Adult Board (SAB) website.
Any changes to training are incorporated with immediate effect
2.6 The Six Principles that underpin all Adult Safeguarding
Empowerment – People being supported and encouraged to make their own decision and informed consent
“I am asked what I want from the safeguarding process and these directly inform what happens”
Prevention – It is better to take action before harm occurs.
“I receive clear and simple information about what abuses, how to recognise the signs and what I can do to seek help.”
Proportionality – The least intrusive response appropriate to the risk presented
“I am sure that the professionals will work in my interest, as I see them and they will only get involved as much as needed.”
Protection – Support and representation for those in greatest need.
“I get help and support to report abuse and neglect. I get help so that I am able to take part in the safeguarding process to the extent to which I want.
Partnership – Local solutions through services working with their communities have a part to play in preventing, deleting and reporting neglect and abuse.
“I know that staff treat any personal or sensitive information in confidence, only sharing what is helpful and necessary. I am confident that professionals will work together and with me to get the best result for me.”
Accountability – Accountability and transparency in delivering safeguarding. “I understand the role of everyone involved in my life and so do they.”
These principles apply to all sectors and settings including care and support services, further education colleges, commissioning, regulation and provision of health and care services, social work, healthcare welfare benefits housing wider local authority function and the criminal justice system. The principles should inform the ways in which professionals and other staff work with adults. They can also help SABs and other organisation more widely, by using them to examine and improve their local arrangements. In addition to these principles the Act seeks to broaden a community approach to establishing their safeguarding arrangements. It is vital that all organisations recognise that adult safeguarding arrangements are there to protect individuals. We all have different preferences, histories, circumstances and lifestyles so it is unhelpful to prescribe a process that must be followed whenever a concern is raised; and the case study below helps illustrate this.
2.7 Case Study
Two brothers with mild learning disabilities lived in their family home, where they had remained following the death of their parents sometime previously. Large amounts of rubbish had accumulated both in the garden and inside the house, with cleanliness and self-neglect an issue. They had been targeted by fraudsters, resulting in criminal investigation and conviction of those responsible, but the brothers had refused services from adult social care and the case closed.
They had however, a good relationship with their social worker, and as concerns about their health and wellbeing continued, it was decided that the social worker would maintain contact, calling in every couple of weeks to see how they were and offer any help to improve the state of their house, to sell it and moved to a living environment in which practical support could be provided.
3.0 Types of Abuse and Neglect
• Physical abuse – including assault, hitting, slapping, pushing, misuse of medication, restraint or inappropriate physical sanctions.
• Domestic violence – including psychological, physical, sexual, financial, emotional abuse; so, called ‘honour’ based violence.
• Sexual abuse – including rape, indecent exposure, sexual harassment, inappropriate looking or touching, sexual teasing or innuendo, sexual photography, subjection to pornography or witnessing sexual acts, indecent exposure and sexual assault or sexual acts to which the adult has not consented or was pressured into consenting.
• Psychological abuse – including emotional abuse, threats of harm or abandonment, deprivation of contact, humiliation, blaming, controlling, intimidation, coercion, harassment, verbal abuse, cyber bullying, isolation or unreasonable and unjustified withdrawal of services or supportive networks.
• Financial or material abuse – including theft, fraud, internet scamming, coercion in relation to an adult’s financial affairs or arrangements, including in connection with wills, property, inheritance or financial transactions, or the misuse or misappropriation of property, possessions or benefits.
• Modern slavery – encompasses slavery, human trafficking, forced labour and domestic servitude. Traffickers and slave masters use whatever means they have at their disposal to coerce, deceive and force individuals into a life of abuse, servitude and inhumane treatment.
• Discriminatory abuse – including forms of harassment, slurs or similar treatment; because of race, gender and gender identity, age, disability, sexual orientation or religion.
• Organisational abuse – including neglect and poor care practice within an institution or specific care setting such as a hospital or care home, for example, or in relation to care provided in one’s own home. This may range from one off incidents to on-going ill-treatment. It can be through neglect or poor professional practice as a result of the structure, policies, processes and practices within an organisation.
• Neglect and acts of omission – including ignoring medical, emotional or physical care needs, failure to provide access to appropriate health, care and support or educational services, the withholding of the necessities of life, such as medication, adequate nutrition and heating.
• Self-neglect – this covers a wide range of behaviour neglecting to care for one’s personal hygiene, health or surroundings and includes behaviour such as hoarding.
Incidents of abuse may be one-off or multiple and affect one person or more. Professionals and others should look beyond single incidents or individuals to identify patterns of harm, just as the Care Quality Commission, as the regulator of service quality, does when it looks at the quality of care in health and care services. Repeated instances of poor care may be an indication of more serious problems and of what we now describe as organisational abuse. In order to see these patterns, it is important that information is recorded and appropriately shared.
3.1 Patterns of Abuse
• serial abusing in which the perpetrator seeks out and ‘grooms’ individuals. Sexual abuse sometimes falls into this pattern as do some forms of financial abuse.
• long-term abuse in the context of an ongoing family relationship such as domestic violence between spouses or generations or persistent psychological abuse; or
• opportunistic abuse such as theft occurring because money or jewellery has been left lying around.
Domestic abuse
In 2013, the government announced changes to the definition of domestic abuse:
• Incident or pattern of incidents of controlling, coercive or threatening behaviour, violence or abuse… by someone who is or has been an intimate partner or family member regardless of gender or sexuality
• Includes: psychological, physical, sexual, financial, emotional abuse; so called ‘honour’ based violence; Female Genital Mutilation; forced marriage.
• Age range extended down to 16.
Many people think that domestic abuse is about intimate partners, but it is clear that other family members are included and that much safeguarding work (that meets the criteria set out in paragraph 14.2) that occurs at home is, in fact concerned with domestic abuse. This confirms that domestic abuse approaches and legislation can be considered safeguarding responses in appropriate cases.
Within the Serious Crime Act 2015 a new offence of Coercive and Controlling Behaviour intimate and familial Relationships was introduced. This offence will incur a maximum of 5 years imprisonment or a fine or both.
Financial abuse
Financial abuse is the main form of abuse identified by the Office of the Public Guardian both amongst adults and children at risk. Financial recorded abuse can occur in isolation, but as research has shown, where there are other forms of abuse, there is likely to be financial abuse occurring. Although this is not always the case, everyone should also be aware of this possibility.
Where the abuse is by someone who has the authority to manage an adult’s money, the relevant body should be informed, for example, the Office of the Public Guardian for deputies and Department for Work and Pensions (DWP) in relation to appointees.
Internet Scams, Postal Scams and Doorstep Crime are targeted at adults at risk, and all are forms of financial abuse. These scams are becoming ever more sophisticated and elaborate.
• Internet scammers can build very convincing websites
• people can be referred to a website to check the caller’s legitimacy, but this can be a copy of a legitimate website
• postal scams are massed produced letters which are made to look like personal or important documents
• doorstep criminals call unannounced at the adult’s home under the guise of legitimate business and offering to fix are often non-existent problem with their property
• sometimes they pose as a police officer or someone of authority
In all cases this is financial abuse and should always be reported to the local police forces or the local Authority Trading Standard Services for investigating
3.2 Who abuses and Neglects Adults?
Anyone can carry out abuse or neglect, including:
• spouses/partners.
• other family members.
• neighbours;
• friends.
• acquaintances.
• local residents.
• people who deliberately exploit adults they perceive as vulnerable to abuse.
• paid staff or professionals; and
• volunteers and strangers.
While a lot of attention is paid, for example, to targeted fraud or internet scams perpetrated by complete strangers, it is far more likely that the person responsible for abuse is known to the adult and is in a position of trust and power.
3.3 Spotting signs of Abuse and Neglect
Workers across a wide range of organisations need to be vigilant about adult safeguarding concerns in all walks of life including, amongst others in health and social care, welfare, policing, banking, fire and rescue services and trading standards, leisure services, faith groups, and housing. GPs, in particular, are often well-placed to notice changes in an adult that may indicate they are being abused or neglected. Findings from Serious Case Reviews have sometimes stated that if professionals or other staff had acted upon their concerns or sought more information, then death or serious harm might have been prevented. The following example illustrates that someone who might not typically be thought of, in this case the neighbour, does in fact have an important role to play in identifying when an adult is at risk.
3.4 Case study
Mr A is in his 40s, and lives in a housing association flat with little family contact. His mental health is relatively stable, after a previous period of hospitalisation, and he has visits from a mental health support worker. He rarely goes out, but he lets people into his accommodation because of his loneliness. The police were alerted by Mr A’s neighbours to several domestic disturbances. His accommodation had been targeted by a number of local people and he had become subjected to verbal, financial and sometime physical abuse. Although Mr A initially insisted they were his friends, he did indicate he was frightened; he attended a case conference with representatives from adult social care, mental health services and the police, from which emerged a plan to strengthen his own self-protective ability as well as to deal with the present abuse. Mr A has made different arrangements for managing his money so that he does not accumulate large sums at home. A community-based visiting service has been engaged to keep him company through visits to his home, and with time his support worker aims to help get involved in social activities that will bring more positive contacts to allay the loneliness that Mr A sees as his main challenge.
It is important that all staff learn to ask, “Is this safe?” If it’s not, then where are the risks? Can they be managed or mitigated or is an immediate response required.
Anyone can witness or become aware of information suggesting that abuse and neglect is occurring. The matter may, for example, be raised by a worried neighbour (see above case study), a concerned bank cashier, a GP, a welfare benefits officer, a
housing support worker or a nurse on a ward. Primary care staff may be particularly well-placed to spot abuse and neglect, as in many cases they may be the only professionals with whom the adult has contact. The adult may say or do things that hint that all is not well. It may come in the form of a complaint, a call for a police response, an expression of concern, or come to light during a need’s assessment. Regardless of how the safeguarding concern is identified, everyone should understand what to do, and where to go locally to get help and advice. It is vital that professionals, other staff and members of the public are vigilant on behalf of those unable to protect themselves. This will include:
• knowing about different types of abuse and neglect and their signs.
• supporting adults to keep safe.
• knowing who to tell about suspected abuse or neglect; and
• supporting adults to think and weigh up the risks and benefits of different options when exercising choice and control.
Awareness campaigns for the general public and multi-agency training for all staff will contribute to achieving these objectives.
4.0 The Mental Capacity Act 2005
People must be assumed to have capacity to make their own decisions and be given all practicable help before anyone treats them as not being able to make their own decisions. Where an adult is found to lack capacity to make a decision then any action taken, or any decision made for, or on their behalf, must be made in their best interests.
Professionals and other staff need to understand and always work in line with the Mental Capacity Act 2005 (MCA). They should use their professional judgement and balance many competing views. They will need considerable guidance and support from their employers if they are to help adults manage risk in ways and put them in control of decision making if possible.
Regular face-to-face supervision from skilled managers is essential to enable staff to work confidently and competently in difficult and sensitive situations.
Mental capacity is frequently raised in relation to adult safeguarding. The requirement to apply the MCA in adult safeguarding enquiries challenges many professionals and requires utmost care, particularly where it appears an adult has capacity for making specific decisions that nevertheless places them at risk of being abused or neglected.
The MCA created the criminal offences of ill-treatment and wilful neglect in respect of people who lack the ability to make decisions. The offences can be committed by anyone responsible for that adult’s care and support paid staff but also family carers as well as people who have the legal authority to act on that adult’s behalf (i.e. persons with power of attorney or Court-appointed deputies).
These offences are punishable by fines or imprisonment. Ill-treatment covers both deliberate acts of ill-treatment and also those acts which are reckless which results in ill-treatment. Wilful neglect requires a serious departure from the required standards of treatment and usually means that a person has deliberately failed to carry out an act that they knew they were under a duty to perform.
Abuse by an attorney or deputy: If someone has concerns about the actions of an attorney acting under a registered Enduring Power of Attorney (EPA) or Lasting Power of Attorney (LPA), or a Deputy appointed by the Court of Protection, they should contact the Office of the Public Guardian (OPG). The OPG can investigate the actions of a Deputy or Attorney and can also refer concerns to other relevant agencies.
When it makes a referral, the OPG will make sure that the relevant agency keeps it informed of the action it takes. The OPG can also make an application to the Court of Protection if it needs to take possible action against the attorney or deputy. Whilst the OPG primarily investigates financial abuse, it is important to note that that it also has a duty to investigate concerns about the actions of an attorney acting under a health and welfare Lasting Power of Attorney or a personal welfare deputy. The OPG can investigate concerns about an attorney acting under a registered Enduring or Lasting Power of Attorney, regardless of the adult’s capacity to make decisions.
5.0 Reporting and responding to Abuse and Neglect
It is important to understand the circumstances of abuse, including the wider context such as whether others may be at risk of abuse, whether there is any emerging pattern of abuse, whether others have witnessed abuse and the role of family members and paid staff or professionals.
The circumstances surrounding any actual or suspected case of abuse or neglect will inform the response. For example, it is important to recognise that abuse or neglect may be unintentional and may arise because a carer is struggling to care for another person. This makes the need to take action no less important, but in such circumstances, an appropriate response could be a support package for the carer and monitoring. However, the primary focus must still be how to safeguard the adult. In other circumstances where the safeguarding concerns arise from abuse or neglect deliberately intended to cause harm, then it would not only be necessary to immediately consider what steps are needed to protect the adult but also whether to refer the matter to the police to consider whether a criminal investigation would be required or appropriate.
The nature and timing of the intervention and who is best placed to lead will be, in part, determined by the circumstances. For example, where there is poor, neglectful care or practice, resulting in pressure sores for example, then an employer-led disciplinary response may be more appropriate; but this situation will need additional responses such as clinical intervention to improve the care given immediately and a clinical audit of practice. Commissioning or regulatory enforcement action may also be appropriate.
Early sharing of information is the key to providing an effective response where there are emerging concerns. To ensure effective safeguarding arrangements:
• all organisations must have arrangements in place which set out clearly the processes and the principles for sharing information between each other, with other professionals and the SAB; this could be via an Information Sharing Agreement to formalise the arrangements; and,
• no professional should assume that someone else will pass on information which they think may be critical to the safety and wellbeing of the adult. If a professional has concerns about the adult’s welfare and believes they are suffering or likely to suffer abuse or neglect, then they should share the information with the local authority and, or, the police if they believe or suspect that a crime has been committed.
6.0 Local Authority’s role in carrying out enquiries
Local authorities must make enquiries, or cause others to do so, if they reasonably suspect an adult who meets the criteria at paragraph 14.2 is, or is at risk of, being abused or neglected.
An enquiry is the action taken or instigated by the local authority in response to a concern that abuse, or neglect may be taking place. An enquiry could range from a conversation with the adult, or if they lack capacity, or have substantial difficulty in understanding the enquiry their representative or advocate, prior to initiating a formal enquiry under section 42, right through to a much more formal multi-agency plan or course of action. Whatever the course of subsequent action, the professional concerned should record the concern, the adult’s views and wishes, any immediate action that has been taken and the reasons for those actions.
The purpose of the enquiry is to decide whether or not the local authority or another organisation, or person, should do something to help and protect the adult. If the local authority decides that another organisation should make the enquiry, for example a care provider, then the local authority should be clear about timescales, the need to know the outcomes of the enquiry and what action will follow if this is not done.
What happens as a result of an enquiry should reflect the adult ‘s wishes wherever possible, as stated by them or by their representative or advocate. If they lack capacity it should be in their best interests if they are not able to make the decision and be proportionate to the level of concern.
The adult should always be involved from the beginning of the enquiry unless there are exceptional circumstances that would increase the risk of abuse. If the adult has substantial difficulty in being involved, and where there is no one appropriate to support them, then the local authority must arrange for an independent advocate to represent them for the purpose of facilitating their involvement.
Professionals and other staff need to handle enquiries in a sensitive and skilled way to ensure distress to the adult is minimised. It is likely that many enquiries will require the input and supervision of a social worker, particularly the more complex situations and to support the adult to realise the outcomes they want and to reach a resolution or recovery. For example, where abuse or neglect is suspected within a family or informal relationship it is likely that a social worker will be the most appropriate lead. Personal and family relationships within community settings can prove both difficult and complex to assess and intervene in. The dynamics of personal relationships can be extremely difficult to judge and rebalance. For example, an adult may make a choice to be in a relationship that causes them emotional distress which outweighs, for them, the unhappiness of not maintaining the relationship.
Whilst work with the adult may frequently require the input of a social worker, other aspects of enquiries may be best undertaken by others with more appropriate skills and knowledge. For example, health professionals should undertake enquiries and treatment plans relating to medicines management or pressure sores.
For clarity: Section 42 Enquiries are the mechanism for Safeguarding Enquiries as set out in the Care Act 2014 Chapter 14. It is a legal duty on local authorities to make enquires or causes someone else to make enquiries.
6.1 INFORMATION GATHERING DIAGRAM
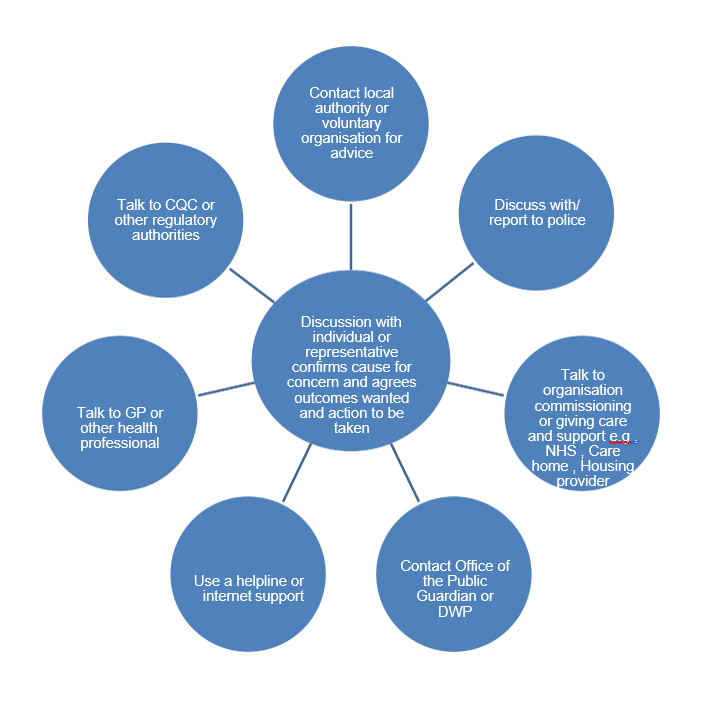
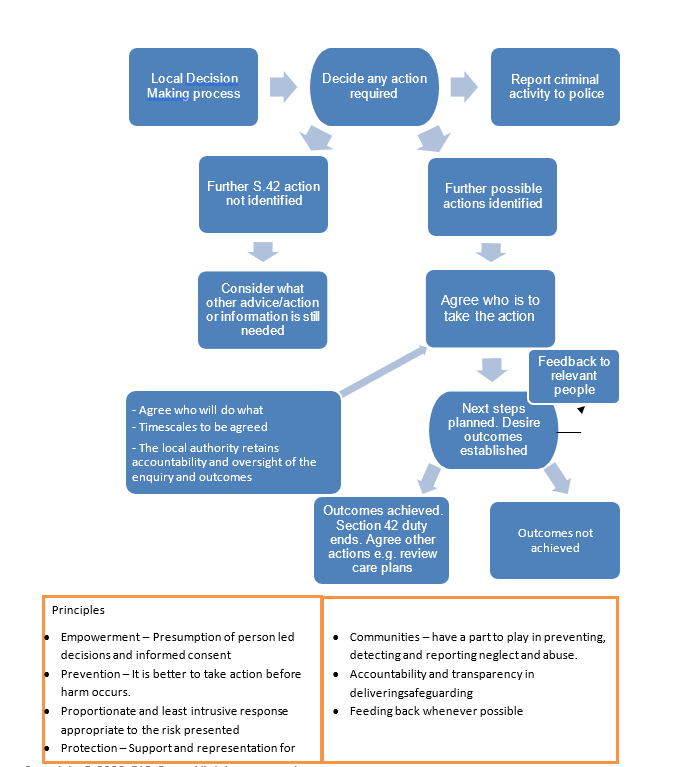
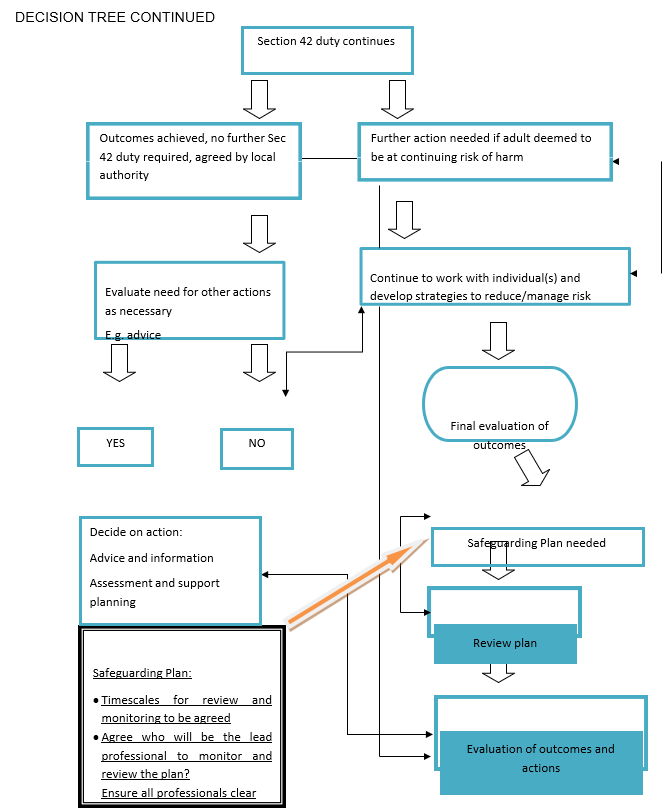
6.2 Report criminal activity to police DECISION MAKING TREE
7.0 Procedures for responding in individual cases
7.1 When should an enquiry take place?
Local authorities must make enquiries, or cause another agency to do so, whenever abuse or neglect are suspected in relation to an adult and the local authority thinks it necessary to enable it to decide what (if any) action is needed to help and protect the adult. The scope of that enquiry, who leads it and its nature, and how long it takes, will depend on the particular circumstances. It will usually start with asking the adult their view and wishes which will often determine what next steps to take. Everyone involved in an enquiry must focus on improving the adult’s well-being and work together to that shared aim. At this stage, the local authority also has a duty to consider whether the adult requires an independent advocate to represent and support the adult in the enquiry. The decision-making tree at highlights appropriate pauses for reflection, consideration and professional judgment and reflects the different routes and actions that might be taken.
Objectives of an enquiry
The objectives of an enquiry into abuse or neglect are to:
• establish facts;
• ascertain the adult’s views and wishes;
• assess the needs of the adult for protection, support and redress and how they might be met;
• protect from the abuse and neglect, in accordance with the wishes of the adult;
• make decisions as to what follow-up action should be taken with regard to the person or organisation responsible for the abuse or neglect; and
• enable the adult to achieve resolution and recovery
The first priority should always be to ensure the safety and well-being of the adult. The adult should experience the safeguarding process as empowering and supportive. Practitioners should wherever practicable seek the consent of the adult before taking action. However, there may be circumstances when consent cannot be obtained because the adult lacks the capacity to give it, but it is in their best interests to undertake an enquiry. Whether or not the adult has capacity to give consent, action may need to be taken if others are or will be put at risk if nothing is done or where it is in the public interest to take action because a criminal offence has occurred. It is the responsibility of all staff and members of the public to act on any suspicion or evidence of abuse or neglect and to pass on their concerns to a responsible person or agency.
Please also refer to Protocols used in Safeguarding Adults Board (osab.co.uk) please amend to you area
“…where a competent adult explicitly refuses any supporting intervention, this should normally be respected. Exceptions to this may be where a criminal offence may have taken place or where there may be a significant risk of harm to a third party. If, for example, there may be an abusive adult in a position of authority in relation to other vulnerable adults (sic), it may be appropriate to breach confidentiality and disclose information to an appropriate authority. Where a criminal offence is suspected, it may also be necessary to take legal advice. Ongoing support should also be offered. Because an adult initially refuses the offer of assistance he or she should not therefore be lost to or abandoned by relevant services. The situation should be monitored and the individual informed that she or he can take up the offer of assistance at any time.”
7.2 Who can carry out an enquiry?
Although the local authority is the lead agency for making enquiries, it may require others to undertake them. The specific circumstances will often determine who the right person to begin an enquiry is. In many cases a professional who already knows the adult will be the best person. They may be a social worker, a housing support worker, a GP or other health worker such as a community nurse. The local authority retains the responsibility for ensuring that the enquiry is referred to the right place and is acted upon. The local authority, in its lead and coordinating role, should assure itself that the enquiry satisfies its duty under section 42 to decide what action (if any) is necessary to help and protect the adult and by whom and to ensure that such action is taken when necessary. In this role if the local authority has asked someone else to make enquiries, it is able to challenge the body making the enquiry if it considers that the process and/or outcome is unsatisfactory.
Where a crime is suspected, and referred to the police, then the police must lead the criminal investigations, with the local authority’s support where appropriate, for example by providing information and assistance. The local authority has an ongoing duty to promote the wellbeing of the adult in these circumstances.
7.3 Case study
Mr A is 24 and has autism and a mild learning disability. He is a very friendly and sociable young man who is prone to waving and talking to most people he comes across, seeing everyone as a potential friend. However, due to his disabilities, he struggles to read the intentions of others and is easily led astray and manipulated. He lives next door to a pub, where he knows the staff and the regulars. He also lives close to his GP and is able to access his most frequently visited places. He does, however, like to walk into town to talk to people he meets out and about. On such occasions, he has been repeatedly tricked into stealing items from a newsagent by a group of teenagers and given large amounts of money away to strangers he strikes up conversations with.
Due to his previous experiences, Mr A was identified during a needs assessment as being at risk of abuse and neglect. A safeguarding enquiry was triggered. The council found that, although Mr A was not currently experiencing abuse or neglect, he remained highly vulnerable to abuse due to his disabilities. To assure his safety in the future, a safeguarding plan was agreed between Mr A and a social worker. This focused on developing his social skills and understanding of relationships and boundaries and the social worker worked with Mr A to consider various support options such as having a buddy or circle of support. The social worker put Mr A in touch with an autism social group which provided sessions on skills for staying safe. As the group was based in town, Mr A’s plan also included a support worker to accompany him. After the first 5 sessions Mr A was able to attend himself but continued to meet with his support worker on a monthly basis as part of the risk management strategy set out in his safeguarding plan.
7.4 What happens after an enquiry?
Once the wishes of the adult have been ascertained and an initial enquiry undertaken, discussions should be undertaken with them as to whether further enquiry is needed and what further action could be taken.
That action could take a number of courses: it could include disciplinary, complaints or criminal investigations or work by contracts managers and CQC to improve care standards. Those discussions should enable the adult to understand what their options might be and how their wishes might best be realised. Social workers must be able to set out both the civil and criminal justice approaches that are open and other approaches that might help to promote their wellbeing, such as therapeutic or family work, mediation and conflict resolution, peer or circles of support. In complex domestic circumstances, it may take the adult some time to gain the confidence and self-esteem to protect themselves and take action and their wishes may change. The police, health service and others may need to be involved to help ensure these wishes are realised.
7.5 Safeguarding Plans
Once the facts have been established, a further discussion of the needs and wishes of the adult is likely to take place. This could be focused safeguarding planning to enable the adult to achieve resolution or recovery, or fuller assessments by health and social care agencies (e.g. a needs assessment under the Care Act). This will entail joint discussion, decision taking and planning with the adult for their future safety and well-being. This applies if it is concluded that the allegation is true or otherwise, as many enquiries may be inconclusive.
The local authority must determine what further action is necessary. Where the local authority determines that it should itself take further action (e.g. a protection plan), then the authority would be under a duty to do so.
The MCA is clear that local authorities must presume that an adult has the capacity to make a decision until there is a reason to suspect that capacity is in some way compromised; the adult is best placed to make choices about their wellbeing which may involve taking certain risks. Of course, where the adult may lack capacity to make decisions about arrangements for enquiries or managing any abusive situation, then their capacity must always be assessed and any decision made in their best interests. If the adult has the capacity to make decisions in this area of their life and declines assistance, this can limit the intervention that organisations can make. The focus should therefore be, on harm reduction. It should not however limit the action that may be required to protect others who are at risk of harm. The potential for ‘undue influence’ will need to be considered if relevant. If the adult is thought to be refusing intervention on the grounds of duress, then action must be taken.
In order to make sound decisions, the adult’s emotional, physical, intellectual and mental capacity in relation to self-determination and consent and any intimidation, misuse of authority or undue influence will have to be assessed.
8.0 Information sharing
8.1 Record-keeping
Good record keeping is a vital component of professional practice. Whenever a complaint or allegation of abuse is made, all agencies should keep clear and accurate records and each agency should identify procedures for incorporating, on receipt of a complaint or allegation, all relevant records into a file to record all action taken. When abuse or neglect is raised managers need to look for past incidents, concerns, risks and patterns. We know that in many situations, abuse and neglect arise from a range of incidents over a period of time. In the case of providers registered with CQC, records of these should be available to service commissioners and the CQC so they can take the necessary action.
Staff should be given clear direction as to what information should be recorded and in what format. The following questions are a guide:
• What information do staff need to know in order to provide a high-quality response to the adult concerned?
• What information do staff need to know in order to keep adults safe under {{org_field_name}}’s duty to protect people from harm?
• What information is not necessary?
• What is the basis for any decision to share (or not) information with a third party?
Records should be kept in such a way that the information can easily be collated for local use and national data collections.
{{org_field_name}} should identify arrangements, consistent with principles and rules of fairness, confidentiality and data protection for making records available to those adults affected by, and subject to, an enquiry. If the alleged abuser is using care and support themselves, then information about their involvement in an adult safeguarding enquiry, including the outcome, should be included in their case record. If it is assessed that the individual continues to pose a threat to other people, then this should be included in any information that is passed on to service providers or other people who need to know.
In order to carry out its functions, SABs will need access to information that a wide number of people or other organisations may hold. Some of these may be SAB members, such as the NHS and the police. Others will not be, such as private health and care providers or housing providers/housing support providers or education providers.
In the past, there have been instances where the withholding of information has prevented organisations being fully able to understand what “went wrong” and so has hindered them identifying, to the best of their ability, the lessons to be applied to prevent or reduce the risks of such cases reoccurring. If someone knows that abuse or neglect is happening, they must act upon that knowledge and not wait to be asked for information.
A Safeguarding Adults Board (SAB) may request a person to supply information to it or to another person. The person who receives the request must provide the information provided to the SAB if:
• the request is made in order to enable or assist the SAB to do its job;
• the request is made of a person who is likely to have relevant information and then either:
I. the information requested relates to the person to whom the request is made and their functions or activities or;
II. the information requested has already been supplied to another person subject to a SAB request for information.
8.2 Confidentiality
{{org_field_name}} should draw up a common agreement relating to confidentiality and setting out the principles governing the sharing of information, based on the welfare of the adult or of other potentially affected adults. Any agreement should be consistent with the principles set out in the Caldicott Review published 2013 ensuring that:
• information will only be shared on a ‘need to know’ basis when it is in the interests of the adult;
• confidentiality must not be confused with secrecy;
• informed consent should be obtained but, if this is not possible and other adults are at risk of abuse or neglect, it may be necessary to override the requirement; and
• it is inappropriate for agencies to give assurances of absolute confidentiality in cases where there are concerns about abuse, particularly in those situations when other adults may be at risk.
Where an adult has refused to consent to information being disclosed for these purposes, then practitioners must consider whether there is an overriding public interest that would justify information sharing (e.g. because there is a risk that others are at risk of serious harm) and wherever possible, the appropriate Caldicott Guardian should be involved.
Decisions about who needs to know and what needs to be known should be taken on a case by case basis, within agency policies and the constraints of the legal framework.
Principles of confidentiality designed to safeguard and promote the interests of an adult should not be confused with those designed to protect the management interests of an organisation. These have a legitimate role but must never be allowed to conflict with the welfare of an adult. If it appears to an employee or person in a similar role that such confidentiality rules may be operating against the interests of the adult, then a duty arises to make full disclosure in the public interest.
In certain circumstances, it will be necessary to exchange or disclose personal information which will need to be in accordance with the law on confidentiality and Data Protection Legislation where this applies. {{org_field_name}} Office and the Office of the Information Commissioner have issued general guidance on the preparation and use of information sharing protocols.
8.3 Front line Staff
Operational front-line staff are responsible for identifying and responding to allegations of abuse and substandard practice. Staff at operational level need to share a common view of what types of behaviour may be abuse or neglect and what to do as an initial response to a suspicion or allegation that it is or has occurred. This includes GPs. It is employers’ and commissioners’ duty to set these out clearly and reinforce regularly.
It is not for front line staff to second-guess the outcome of an enquiry in deciding whether or not to share their concerns. There should be effective and well-publicised ways of escalating concerns where immediate line managers do not take action in response to a concern being raised.
Concerns about abuse or neglect must be reported whatever the source of harm. It is imperative that poor or neglectful care is brought to the immediate attention of managers and responded to swiftly, including ensuring immediate safety and well- being of the adult. Where the source of abuse or neglect is a member of staff it is for the employer to take immediate action and record what they have done and why (similarly for volunteers and or students).
There should be clear arrangements in place about what each agency should contribute at this level. These will cover approaches to enquiries and subsequent courses of action. The local authority is responsible for ensuring effective co-ordination at this level.
Case study
A service user in her own home told the district nurse that staff members spoke disrespectfully to her and that there were episodes of her waiting a long time for the staff to assist with toileting. The care agency user was very unhappy with the treatment she was receiving and was regularly distressed and tearful. The care agency user was reluctant for a formal safeguarding enquiry to take place but did agree that the issues could be discussed with the manager. The district nurse negotiated some actions with the manager to promote good practice and address the issues that had been raised. When the district nurse reviewed the situation; the manager of the care agency had dealt with the issues appropriately and devised an action plan. The care agency user stated that she was now happy – staff ‘couldn’t be more helpful’.
Set out below is {{org_field_name}}’s response to the changes explained above. It is important to emphases the evolving nature of these changes, in particular, the relevance of local authority issued guidance and the impact on providers generally. It is therefore essential that this policy is developed, reviewed and amended as necessary to ensure that all guidance is fully understood and embedded within this policy.
9.0 Safeguarding Adult Boards (SABs)
Local authorities have begun to implement some of the changes and Safeguarding Adult Boards (SABs) have been set up locally. Each SAB will be set up via their local authority and therefore the mechanisms may be different. They are the strategic arm of the safeguarding team and have three core duties:
- It must publish a strategic plan for each financial year that sets out how it will meet its main objective and what the members will do to community involvement, and the SAB must consult with the local Healthwatch organisation.
The plan must be evidence based and make use of all available evidence and intelligence from partners to form and develop its plan.
- It must publish an annual report detailing what the SAB has done during the year to achieve its main objective and implement its strategic plan, and what each member has done to implement the strategy as well as detailing the finding of any safeguarding Adult Reviews (SARs) and subsequent action.
- It must conduct any Safeguarding Action Review in accordance with Section 44 of the Act
The collaboration and cooperation of all partner agencies, including providers is core to the guidance including relevant information sharing when requested.
9.1 Safeguarding Adult’s Reviews (SARs)
SABs must arrange a SAR when an adult in its area dies as a result of abuse or neglect, whether known or suspected, and there is concern that partner agencies could have worked more effectively to protect the adult.
SABs must also arrange a SAR if an adult in its area has not died, but the SAB knows or suspects that the adult has experienced serious abuse or neglect. In the context of SARs, something can be considered serious abuse or neglect where, for example the individual would have been likely to have died but for an intervention or has suffered permanent harm or has reduced capacity or quality of life (whether because of physical or psychological effects) as a result of the abuse or neglect. SABs are free to arrange for a SAR in any other situations involving an adult in its area with needs for care and support.
The SAB should be primarily concerned with weighing up what type of ‘review’ process will promote effective learning and improvement action to prevent future deaths or serious harm occurring again. This may be where a case can provide useful insights into the way organisations are working together to prevent and reduce abuse and neglect of adults. SARs may also be used to explore examples of good practice where this is likely to identify lessons that can be applied to future cases.
The Policy
- Making Enquiries
Making enquiries is the term now used as a response to any adult safeguarding concern and the following procedures are in place for all staff who need to report an adult safeguarding concern. As new guidance is issued by our local authority partners, based on the new framework for Adult Safeguarding within the Care Act 2014, becomes available the current guidance issued by {{org_field_name}} has been amended to reflect the new regulatory framework which is detailed in Chapter 14 of the Care and Support Statutory Guidance October 2014.
10.1 Staff – How to report a Safeguarding Concern
Any suspicion of a safeguarding situation must be reported as a matter of course, to the Register Management or in their absence, to the senior manager on duty at the time.
It is your duty to report any such allegation and the appropriate manager will then take advice and follow the appropriate guidance. If the safeguarding concern involves the manager, the report should be made to the Director / Nominated Individual who will then take advice and follow the appropriate guidance.
The requirement is to report an allegation and if there is anything else required from the staff member reporting the allegation this will be requested as appropriate.
It is good practice, as soon as is possible for contemporaneous notes to be recorded for future reference.
Where required, support should be given to the staff member dependent upon the situation, their response and the urgency of the situation.
To report a safeguarding concern should you chose not to report to the Registered Manager or Nominated Individual in the first instance, please refer to:
Local Adult Safeguarding Authority: {{org_field_local_authority_information_link}}
Phone number for the local Adult Safeguarding Authority: {{org_field_local_authority_phone_number}}
- Telephone: 03000 616161
- Email: enquiries@cqc.org.uk
- Write to: CQC National Correspondence Citygate Gallowgate Newcastle upon Tyne NE1 4PA
- Online at: www.cqc.org.uk/GiveFeedback
Refer to: Raising a concern with CQC: A quikc guide for health and care staff about whistleblowing
Remember if you think a crime has been committed please contact the police via 111 or 999
- Service Users – how to report a safeguarding concern
During the information gathering process within our quality assurance systems service users and or their representatives need to be informed and asked about any inappropriate behaviour verbal or physical that they have observed or been subject to by staff or visitors. This needs to be handled in a sensitive manner.
As part of the information given to new service users and or their representatives our Service User Guide explains and details how to report a safeguarding concern.
Information on raising a safeguarding concern can also be found on notice boards at the office.
Service Users and or their representatives can inform any staff on duty at any time of their concerns. Staff will then report to the designated manager.
10.3 The Role of the Manager
As immediate assessment of the incident should be undertaken by the manager (Safeguarding Lead) in relation to the following:
- The health safety and wellbeing of the adult.
- Their mental capacity to understand comprehend and make decisions regarding the actions to be considered.
- Their needs preference and wishes concerning any action to be considered.
From this assessment, the manager will then take further advice from the Local Safeguarding Team or, institute steps to ensure the protection and safeguarding of the adult; as appropriate; with immediate effect.
The manager, in this context, is the person to whom the concern has been reported to, whether during office hours or out of hours. They will be the Responsible Manager until they are informed otherwise. Records and notes of all actions should be taken. This includes any advice given to the Responsible Manager by any triage arrangements that are in place.
10.4 The Role of the Local Authority
All local authorities have a legal duty to make enquiries or cause another agency to do so, whenever abuse or neglect are suspected in relation to an adult. The nature, scope, how long it takes and who leads it will depend on the particular circumstances presented. Everyone involved in an enquiry must focus on improving the adult’s wellbeing and work together to that shared aim. The objectives of the enquiry are to:
It is important to recognise that any member of staff involved in a safeguarding situation can find it stressful and distressing and workplace support should be available
• Establish fact;
• Ascertain the Adult’s views and wishes;
• Assess the needs of the adult for protection, support and redness and how they might be met;
• Protect from abuse and neglect, in accordance with the wishes of the adult;
• Make decisions as to what follow up action should be taken with regard to the person or organisation responsible for the abuse or neglect; and
• Enable the adult to achieve resolution and recovery
The first priority must always be to ensure the safety and wellbeing of the adult. It is the responsibility of all staff and members of the public to act on any suspicion or evidence of concerns to a responsible person or agency.
Please note the following:
“Where a competent adult explicitly refuses any supporting intervention, this should normally be respected. Exceptions to this may be where or criminal offence may have taken place or where there may be a significant risk of harm to a third party. If for example, there may be an abuse adult in a position of authority in relation to other vulnerable adults (sic), it may be appropriate to breach confidentiality and disclose information to on appropriate authority. Where criminal offence is suspected it may also be necessary, to take further advice. Ongoing support should also be offered. Because an adult initially refuses the offer of assistance they should not therefore be lost to or abandoned by relevant services. The situation should be monitored and the individual informed that they can take up the offer of assistance at any time.
11.0 Statutory Notifications to CQC
A Statutory Notification is sent to CQC concerning any abuse or alleged abuse involving a person(s) using our service. This includes where the person(s) is either the victim(s) or the abuser(s), or both. We notify CQC about abuse or alleged abuse at the same time as alerting our local safeguarding authority for children or adults, and the police where a crime has been or may have been committed.
The person submitting the Statutory Notification must use the electronic form supplied on CQC website to notify both alleged and actual abuse and email the form to CQC at the address stated on the form: https://www.cqc.org.uk/guidance-providers/notifications
Providers Guidance -Statutory Notifications for non-NHS trust providers
The CQC website is regularly checked to ensure the above guidance we use is up to date.
12.0 Restrictive Interventions
This policy and our organisational responses to restrictive practices reflects the guidelines in the document below.
Positive and Proactive Care: reducing the need for restrictive interventions Prepared by the Department of Health. Published in April 2014.
This guidance is of particular significance for health and social care services where individuals who are known to be at risk of being exposed to restrictive interventions are cared for. Such settings may provide services to people with mental health conditions, autistic spectrum conditions, learning disability, dementia and/or personality disorder, older people and detained patients. It is more broadly applicable across general health and social care settings where people using services may on occasion present with behaviour that challenges but which cannot reasonably be predicted and planned for on an individual basis. This may include homes where
individuals employ their own support staff, and community-based primary and secondary care settings.
Related Policies
Challenging Behaviour, Violence and Aggression Confidentiality
Data Protection Legislative Framework (GDPR) Deprivation of Liberty Safeguards
Duty of Candour
Handling of Service Users Money Mental Capacity Act 2005 Record Keeping
Whistleblowing
Related Guidance
For Local Authority Multi-Agency Adult Safeguarding Guidance/ Protocol please refer to your local area
- Care Act 2014 Safeguarding Adults: https://www.legislation.gov.uk/ukpga/2014/23/enacted
- SCIE-Safeguarding Adults Reviews / SARs under the Care Act
- Older people with social care needs and multiple long-term conditions [NG 22] Published November 2015 https://www.nice.org.uk/guidance/ng22
- Social Care for older people with multiple long-term conditions QS132: https://www.nice.org.uk/guidance/qs132
· Whistleblowing
The government has set up a whistle blowing helpline for NHS and Social care. This is available to both managers for advice and staff for reporting purposes. This telephone number is 08000 724 725.
CQC whistleblowing “Guidance for providers who are registered with CQC”
· Care Quality Commission (CQC)
Citygate Gallowgate
Newcastle Upon Tyne NE1 4PA
Training Statement
All staff will be made aware of the changes outlined above. This will include the Multi- Agency Safeguarding Agreement from the local authority, as amended. All staff, during induction are made aware of {{org_field_name}}’s policies and procedures, all of which are used for training updates. All policies and procedures are reviewed and amended where necessary and staff are made aware of any changes. Observations are undertaken to check skills and competencies. Various methods of training are used including one to one, on-line, workbook, group meetings, individual supervisions and external courses are sourced as required.
Responsible Person: {{org_field_registered_manager_first_name}} {{org_field_registered_manager_last_name}}
Reviewed on: {{last_update_date}}
Next review date: this policy is reviewed annually (every 12 months). When needed, this policy is also updated in response to changes in legislation, regulation, best practices, or organisational changes.
Copyright ©2024 {{org_field_name}}. All rights reserved